


Healthcare consumes 18% of the U.S. gross domestic product—$2.7 trillion. According to Ameed Ali, PharmD, you’d have to run a ribbon of $100 bills from Earth to the moon and back five times to reach $2.7 trillion. That’s a lot of Benjamins. Even more startling is that 30% of that cost—$800 billion—is waste.
Ali, Assistant Professor of Pharmacy and Therapeutics, University of Pittsburgh School of Pharmacy, spoke last month at the American College of Healthcare Architects/AIA Academy of Architecture for Health Summer Leadership Summit, in Chicago. The annual ACHA/AAH Summit focuses on the business of healthcare—how economic factors can impact the design and construction of hospitals, clinics, and other medical facilities.
That $800 billion in waste (based on a 2012 estimate by the Institute of Medicine) includes $210 billion in unnecessary services (for example, unneeded lab tests), $190 billion in excessive administrative costs, $130 billion in inefficiently delivered services, $105 billion from “too-high prices,” and $55 billion from missed prevention opportunities. Fraud, the traditional whipping boy, accounts for less than one-tenth of waste, $75 billion, said Ali.
ALSO SEE: Healthcare designers get an earful about controlling medical costs. Read the article.
At the current pace, in 2020 the U.S. will spend $4.2 trillion a year on healthcare; unchecked, waste would hit $1.2 trillion. Yet “waste” is keeping a lot of poorly performing hospitals in business, said Ali. Currently, one in five Medicare patients has to go back to the hospital within 30 days because the original procedure failed. Hospitals make 20% of their revenues on readmissions, but when the Affordable Care Act kicks in next year, Medicare will start cutting payments for readmissions. “The 30-day readmission rate is very high on a hospital CEO’s mind,” Ali told ACHA/AAH members.
'Zero defects' in healthcare
Taking the “defect rate” in healthcare down to zero was the theme of a riveting talk by Gary S. Kaplan, MD, Chair/CEO of Virginia Mason Medical Center, a nonprofit healthcare system in Seattle with nine facilities (including a 336-bed teaching hospital), 500 physicians, and 5,000 employees.
12 healthcare projects honored at ACHA/AAH Leadership Summit
Recipients of the AIA Academy of Architecture for Health’s AIA National Healthcare Design Awards were honored at the ACHA/AAH Summer Leadership Summit. The awards program showcases the best of healthcare building design and healthcare design-oriented research. Projects exhibited conceptual strengths that solve aesthetic, civic, urban, and social concerns as well as the requisite functional and sustainability concerns of a hospital.
Recipients were selected in five categories: 1) Built, <$25 million in construction cost; 2) Built, >$25 million in construction cost; 3) Unbuilt; 4) Innovations in Planning and Design Research; and 5) Master Planning Urban Design for Healthcare Settings.
Jurors for the 2013 National Healthcare Design Awards: Joan Saba, AIA, Chair, NBBJ; Orlando T. Maione, AIA, Maione Associates; Mike Mense, FAIA, mmenseArchitects; Kathy Reno, Joint Commission Resources, Inc.; Bill Rostenberg, FAIA, Stantec; Bryan Shiles, AIA, WRNS; and Ron Smith, AIA, Design At The Intersection.
In 2000, the hospital, founded in 1920 on the Mayo Clinic group practice model, was losing millions. Morale was at a low point; employee retention was slipping. “We realized that our processes were designed around us—the doctors, nurses, and administrators—not around the patient,” said Kaplan. At a meeting of the entire professional staff, he issued a terse directive: “We change, or we die.”
Since then, Kaplan has led 13 research missions to Toyota manufacturing facilities in Japan to learn how to apply the automaker’s “lean” principles to healthcare. These trips, each involving 25 to 30 physicians, nurses, and staff, have resulted in 1,300 “improvement events” in VMMC processes.
Through its Value Stream Development system, VMMC found that nurses were spending 60-70% of their time searching for supplies or tracking down patients. Process improvements led to changes that enable nurses to spend 90% of their time with patients. The 5S process—for “sort, simplify, standardize, sweep, self-discipline”—replaced multiple anesthesia “shadow boards” (the tray that holds the anesthesiologist’s supplies) with a single standard board, improving safety and efficiency while cutting costs.
One controversial change involved adopting the Toyota procedure that allows any worker to “stop the line” without fear of retribution if he or she spots a problem. “Some of our people complained that cars aren’t people,” said Kaplan. True, said Kaplan, but patient safety had to come first.
In 2002, VMMC adopted its trademarked Patient Safety Alert Process, which empowers any employee to report a patient safety alert 24 hours a day, with a management commitment to “drop and run” to address the question immediately. Since then, 32,380 alerts—about eight or nine a day—have been issued. Only a small number have been serious in nature, but many have led to improvements. In fact, VMMC’s “obsession with safety” has resulted in its physician liability costs being cut in half, in a state with no medical tort reform.
VMMC has also cut the cost of care for Seattle-area employers. Since 2007, Boeing has referred employees with chronic diseases like diabetes and back, shoulder, and hip pain to Virginia Mason. The target: cut medical costs by 15%. In fact, Boeing’s costs went down by 33%. No wonder Costco, Microsoft, Starbucks, and King County have asked for similar programs for their workers. And last January, Walmart designated VMMC as one of only six medical centers in the U.S. to serve as a “Walmart Center of Excellence”—in VMMC’s case, for heart and complex spine care.
Trimming waste and unnecessary costs through improved processes while keeping patient needs first will carry over to better facility design, provided design teams “engage the people who do the work,” Kaplan told ACHA/AAH attendees. “It’s not ‘Form follows function.’ It’s ‘Better form follows improved function,’” he said.
Putting Building Teams to work to help control medical costs
The key takeaway from the ACHA/AAH Summit is that Building Teams that specialize in healthcare facilities need to do their part to control costs. George R. Tingwald, MD, AIA, Director of Medical Planning at Stanford Hospital and Clinics, told how only three change orders were issued in the completion of SHC’s Byers Eye Institute, in Redwood City, Calif., thanks to the use of BIM. “We used to get a thousand change orders on a project like that,” said the physician/architect.
With the Affordable Care Act about to kick in on January 1, healthcare providers—and their design and construction partners—will need to address what Kevin Vigilante, MD, Senior Vice President, Booz Allen Hamilton, called the “triple aim” of 1) improving the quality and experience of care, 2) reducing cost per patient, and 3) improving health at the “population” level.
“Heart disease, stroke, diabetes, cancer, arthritis—these have become population health issues,” he told ACHA/AAH attendees. In the future, improving care for those with chronic conditions may depend much more heavily on technology, such as mobile phones and social networking. “A diabetic has the condition every minute of the year, but may only connect with healthcare providers for a few hours a year,” he said.
There will still be a need for brick-and-mortar facilities, said Vigilante, but “we’re going to need a new paradigm, ‘connected care,’ to provide continuous healing relationships.”
Related Stories
 Campus, the Building Team took advantage of the sites natural coastal g")
| Dec 28, 2014
AIA course: Enhancing interior comfort while improving overall building efficacy
Providing more comfortable conditions to building occupants has become a top priority in today’s interior designs. This course is worth 1.0 AIA LU/HSW.

| Dec 28, 2014
6 trends steering today's college residence halls
University students want more in a residence hall than just a place to sleep. They want a space that reflects their style of living and learning.
")
| Dec 28, 2014
Using energy modeling to increase project value [AIA course]
This course, worth 1.0 AIA LU/HSW, explores how to increase project value through energy modeling, as well as how to conduct quick payback and net present value studies to identify which energy strategies are most viable for the project.
| Dec 28, 2014
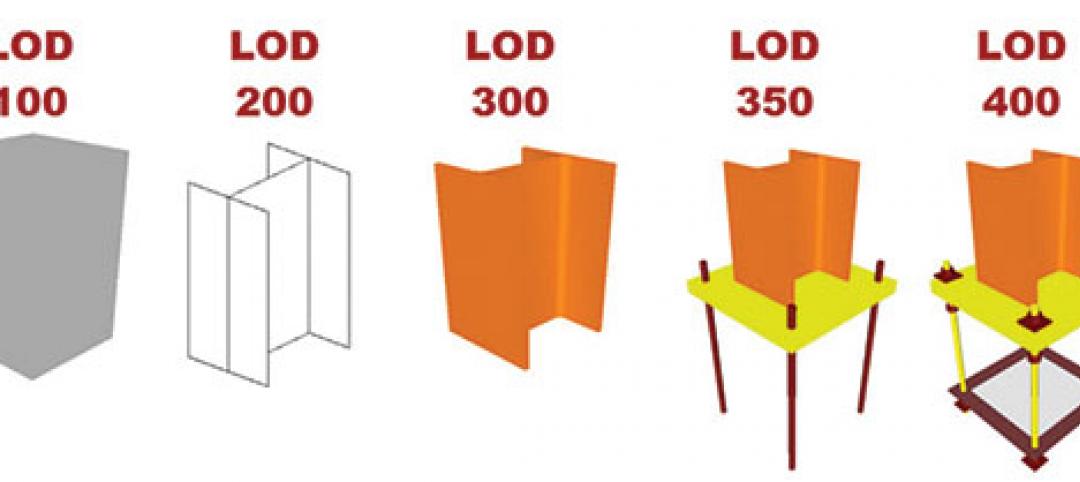
The lowdown on LODs: Bringing clarity to BIM
These days, BIM is par for the course across most facets of design. But a lot of the conversation surrounding BIM still lacks clarity due to ambiguous terminology, a lack of clear-cut guiding illustrations, and widely varying implementation, writes GS&P's John Scannell.

| Dec 28, 2014
The future of airport terminal design: destination status, five-star amenities, stress-free travel
Taking a cue from the hospitality industry, airport executives are seeking to make their facilities feel more like destinations, writes HOK's Richard Gammon.

| Dec 28, 2014
10 key design interventions for a healthier, happier, and more productive workplace
Numerous studies and mountains of evidence confirm what common sense has long suggested: healthy, happier workers are more productive, more likely to collaborate with colleagues, and more likely to innovate in ways that benefit the bottom line, writes Gensler's Kirsten Ritchie.

| Dec 28, 2014
7 fresh retail design strategies
Generic ‘boxes’ and indifferent service won’t cut it with today’s savvy shoppers. Retailers are seeking a technology-rich-but-handmade vibe, plus greater speed to market and adaptability.

| Dec 28, 2014
Workplace design trends: Make way for the Millennials
Driven by changing work styles, mobile technology, and the growing presence of Millennials, today’s workplaces are changing, mostly for the better. We examine the top office design trends.

| Dec 28, 2014
AIA: Commercial glass façade and door systems
When it comes to selecting fenestration systems—particularly glass facades and door systems—a number of factors come into play, requiring a thorough evaluation of a project’s individual requirements.

| Dec 28, 2014
10 essential habits of successful architects
Want to take the next step as a design processional? John Gresko, Senior Project Architect with HDR, explores the traits that many great architects possess.



