


Georgia Tech’s SimTigrate Design Lab and Dräger, an international supplier of medical and safety technology, have released a white paper that sets out to demonstrate the advantages for Intensive Care Units in hospitals of ceiling-mounted beam systems over traditional headwall systems or those operated with articulated arms or overhead booms.
One of this paper’s stated purposes is to understand how medical teams evaluate architectural solutions to medical gas delivery, and to compare user experiences with different overhead utilities in the ICU. Its opinions are based primarily on field observations of the use of booms in three hospitals, interviews with staff in other ICUs who have used the beam system, and a simulation conducted in a low-fidelity mockup with nurses, physicians and respiratory therapists from a hospital undergoing a renovation of its ICU patient rooms.
The paper is also a full-throated endorsement of Dräger’s beam system for ICUs, although it does not delve into cost comparisons among different delivery systems.
The paper observes that operating rooms in most hospitals already favor ceiling-mounted systems to deliver medical gases and supply power. As more patient care is provided at the bedside within ICUs, hospitals have replicated overhead service delivery solutions in those units to realize the same advantages of improved access to the head of the bed.
“Yet it is important to keep in mind that ICU rooms do not function exactly like operating rooms, and therefore may have different needs,” the paper states.
The white paper spells out the disadvantages of headwalls in ICUs (space, patient and equipment access, mobility). It also provides a number of reasons why overhead booms aren’t optimal, either.
For example, while overhead booms free up floor space, “they are quite large and take up a lot of real estate in the patient room.” Due to limited space in most inpatient rooms, nurses routinely have to move both boom arms out of the way to move patients into or out of the room.
The flexibility of articulated boom arms has a downside, too, in that the arms can block critical views of such things as monitors.
Perhaps the biggest disadvantage of booms operating overhead is that they impede the use of patient lifts, because the range of a cross bar is limited by the boom and requires that the boom arms are pushed all the way forward, and the bed be moved further away from the wall, to gain access to the patient’s center of gravity.

These illustrations compare patient access when an ICU room is equipped with a Ponta beam system (top) versus an articulated arm system. The Georgia Tech white paper says the biggest disadvantage of booms operating overhead or to the side of the bed is that they impede the use of patient lifts, because the range of a cross bar is limited by the boom and requires that the boom arms are pushed all the way forward, and the bed be moved further away from the wall, to gain access to the patient’s center of gravity. Image: “Comparison of Overhead Utility Systems for Intensive Care Rooms.”
The bulk of this white paper is devoted to demonstrating the advantages of Dräger’s Ponta overhead beam system within an ICU environment.
It states that the Ponta beam takes up less space than an overhead boom, which is important for smaller inpatient rooms. The beam system allows nurses to move the shuttles (columns that suspend from the beam) laterally to come closer together to support infants in incubators or patients in chairs; or farther apart to support bariatric patients.
The columns are customizable for the specific needs of the ICU clinic and standardized across all rooms, such that the ventilator is always on the same side of the patient bed. The beam system allows staff to move the bed in and out of the room easier.
To back up its claims, Georgia Tech, with support from Dräger, the architectural firm HKS, and Grady Health System, conducted three simulation sessions on the Grady’s campus in downtown Atlanta to give the nurses, providers, and facility leadership an opportunity to try out the Ponta beam under real-life care situations.
A critical care doctor with Grady scripted a complex patient scenario that required bulky equipment, access to the head of the bed, and placed many people in the room.
The participants included nurses, doctors, and leadership from Grady’s medical ICU, as well as nurses from the Marcus Stroke and Neurosciences Center who were familiar with using a boom and could compare the performance of different delivery systems.
The 15 simulation participants who completed surveys rated the Ponta system positively in all categories. A dozen agreed or strongly agreed that the beam reduced clutter around the bed; 13 agreed or strongly agreed that the beam better organizes equipment, and 11 agreed or strongly agreed that the beam system is better for managing cables.
Clear majorities of participants also judged the beam system superior to overhead boom systems for providing better access to the patient and to gases and equipment, and better visibility to monitors.
“It is clear that ceiling-mounted solutions for delivery of utilities are far superior than the traditional headwall,” the report states. But unlike overhead boom systems, which were designed originally for operating rooms, Dräger’s Ponta beam system is specifically desgined for smaller inpatient room. The beam system also minimizes bulky infrastructure directly over the patient.
Perhaps the biggest advantage of the Ponta beam is that because it is not mounted directly over the center of the bed, that space is available for overhead patient lift tracks, making the patient lift more effective and easier to operate, which results in more frequent use.
Related Stories

| Feb 15, 2013
Preservation lawsuit over Chicago's Prentice Hospital dropped
Preservation lawsuit over Chicago's Prentice Hospital dropped, freeing Northwestern University to demolish it and build a new research facility.

| Feb 14, 2013
5 radical trends in outpatient facility design
Building Design+Construction combed the healthcare design and construction sector to evaluate the latest developments in outpatient facility designs. Here are five trends to watch.

| Feb 14, 2013
Peter Bardwell named 2013 president of the American College of Healthcare Architects
The Board of Regents of the American College of Healthcare Architects (ACHA) has named Peter L. Bardwell, FAIA, FACHA of Columbus, Ohio as 2013 national President.

| Feb 6, 2013
George W. Bush Presidential Center among award-winning roofing projects honored by Sika Sarnafil
Winners of the 2012 Contractor Project of the Year Competition were announced this week by Sika Sarnafil. The annual competition highlights excellence in roofing installation. Roofing contractors are judged based on project complexity, design uniqueness, craftsmanship, and creative problem solving.

| Feb 6, 2013
RSMeans cost comparisons: office buildings and medical offices
RSMeans' February 2013 Cost Comparison Report breaks down the average construction costs per square foot for four types of office buildings across 25 metro markets.
| Dec 9, 2012
AEC professionals cautiously optimistic about commercial construction in ’13
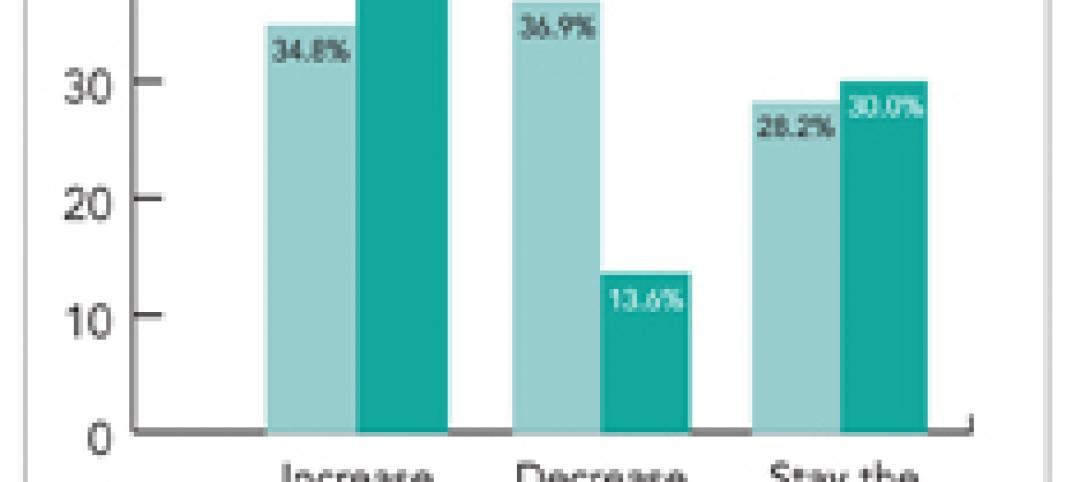
Most economists say the U.S. is slowly emerging from the Great Recession, a view that was confirmed to some extent by an exclusive survey of 498 BD+C subscribers whose views we sought on the commercial construction industry’s outlook on business prospects for 2013.

| Nov 11, 2012
Greenbuild 2012 Report: Healthcare
Green medical facilities extend beyond hospital walls

| Oct 24, 2012
Loma Linda University Medical Center lets light in with metal wall systems
Designers for the building aimed to create a positive environment for patients and visitors, and wanted to let in as much natural daylight as possible.

| Oct 11, 2012
Hank Adams Named to Lead HDR’s Healthcare Program
With more than 25 years of experience, HDR vice president is tapped to lead firm's healthcare projects.



